
How to Implement Value-Based Care
Value-based care is no longer optional. Healthcare costs are rising, regulators are tightening requirements, and both payers and providers are under pressure to deliver better outcomes at lower costs. For executives and IT leaders, the challenge is clear: how to successfully shift from fee-for-service to value-based models without disrupting operations. This guide outlines the essential steps to implement value-based care.
Why shift to value-based care now?
Plainly put, value-based care (VBC) means paying for health outcomes and efficient care, better health at lower total cost, rather than paying for each visit or procedure. The aim is better patient experience, better population health, and lower overall cost. That is CMS’s definition, and the government’s value-based programs are built around that idea.
Why leaders should care now
- Money is moving to VBC. Medicare ACOs in the Shared Savings Program recorded program-record net savings in 2023, proving that VBC models can work at scale. That matters because those savings translate into policy momentum and contracting pressure for payers and providers.
- Technical and regulatory changes reduce friction. Rules for payer data APIs and prior-authorization automation are shifting previously manual processes into machine-readable flows, making it possible to automate many administrative tasks that used to stall care.

Note: By 2030, CMS (Centers for Medicare & Medicaid Services) wants all Medicare payments to be tied to value-based care (VBC). That means paying for better patient outcomes instead of just the number of services provided.
What that means for your organization: VBC is now mostly an execution problem. If you can align contracts, measure outcomes reliably, and change day-to-day workflows, you can capture the financial upside and improve care.
Guide on How to Implement Value-Based Care
How to Assess Your Organization’s Readiness for Value-Based Care
A practical readiness check saves time and prevents wasted investment. Therefore, treat this like a brief audit you can do in 4–6 weeks.
Core areas to review:
- Leadership & governance. Do you have an executive sponsor (CFO, CMO) and a multi-disciplinary steering group? VBC needs quick decisions across finance, quality, IT, and operations.
- Contract and measure inventory. Which contracts do you have (MSSP/ACO, MA, commercial bundles)? Which measures matter (HEDIS, CAHPS, PROMs)? Map them now. NCQA is moving to digital HEDIS (dQMs), which affects how you’ll compute measures.
- Data & technical maturity. EHR versions, API readiness (SMART on FHIR), claims feeds (X12), identity management, and whether you have an MPI. Do you have a plan to use Bulk FHIR for population extracts?
- Operations & staffing. Current care management capacity, case manager ratios, and clinical workflow readiness for embedded tools.
- Security & compliance. A current HIPAA risk analysis and vendor BAAs use NIST SP 800-66 guidance as a practical checklist.
Deliverables from readiness work: prioritized gap list, a 12-month MVP scope, a pilot contract, and a one-page KPI scorecard (quality, utilization, cost, member experience).
Setting Measurable Goals and Patient Segmentation in Value-Based Care
If you can’t measure it, you can’t improve it. Hence, define a compact set of outcome targets and the patient groups you’ll focus on first.
How to pick goals:
- Pick 4–8 starter measures that link to money (e.g., HEDIS diabetes control, BP control, colorectal screening, readmissions) and that you can influence operationally. NCQA’s digital HEDIS work means you can automate many of these calculations once your data flows are in place.
- Add one patient-reported outcome for conditions where function matters (orthopedics, cardiac rehab, behavioral health). ICHOM and PROMIS are the widely used PROM toolsets for outcomes that matter to patients.
- Define financial goals, target shared savings thresholds, revenue protection under risk adjustment (HCC), or reduced denial/authorization lag if you are a payer.
How to segment patients:
- By risk: High-risk (complex chronic + recent ED/hospital), medium risk, and low risk. Risk adjustment via CMS-HCC models protects revenue and helps prioritize who gets high-touch management.
- By condition bundle: Diabetes, CHF, COPD, CKD, start where you have clinical protocols and measurable interventions.
- By social risk: Identify SDOH flags early transportation, food insecurity, housing instability, and include them in targeting logic.
Note: link each measure to a data source of record (EHR, claims, RPM, lab) and name an accountable owner.
Data Integration and Interoperability for Value-Based Care Success
This is the technical backbone. For this reason, without timely, longitudinal data, you can’t attribute care, compute measures, or run risk models.
Standards and connections to prioritize:
- SMART on FHIR: embed clinician-facing apps inside the EHR so clinicians don’t have to toggle systems.
- Bulk FHIR (Flat FHIR): for nightly population extracts to refresh registries and analytics without hammering transactional APIs. Use it for HEDIS/dQM computation and worklist refreshes.
- Da Vinci / HL7 Prior Authorization (PAS): use the Da Vinci guides and the growing ecosystem to automate prior authorization workflows as required by CMS.
- TEFCA / QHINs: TEFCA is bringing nationwide exchange via QHINs; consider an on-ramp through your HIE or vendor to fill outside encounter gaps that break denominators. Over 9,000 orgs have started signing up to participate.
Data engineering priorities:
- Canonical patient timeline merges ADT events, problem lists, meds, labs, claims, and device/RPM feeds into a single view. Use deterministic + probabilistic matching for identity resolution.
- Claims processing ingests 837/835 files, handles late claims and adjustments, and reconciles them against clinical timelines. Claims are essential for cost, utilization, and attribution.
- Lineage & provenance, every quality calculation must show source data and issue date (this builds provider trust and auditability).
- APIs back to workflow surface alerts and tasks to clinician workflows (SMART apps) and care manager dashboards.
Why custom software: off-the-shelf systems rarely map your exact contracts and local connections. A custom interoperability hub lets you normalize vocabularies and maintain a versioned, auditable measure pipeline.
Read more about Healthcare Data Integration for Value-Based Care
Building Analytics and Dashboards to Track Value-Based Care Performance
Analytics turn data into decisions. Therefore, you need two layers: operational work-lists for care teams and strategic dashboards for leadership.
Operational analytics (care team):
- Risk-stratified registries with daily/weekly refresh.
- Worklists and tasks are generated from measurable gaps (e.g., patients missing an A1c test or overdue colonoscopy).
- Closed-loop tasking and time-to-close metrics to show frontline productivity.
Executive analytics (leadership):
- Contract performance: shared savings forecasts, quality scores (HEDIS, CAHPS), utilization trends (ED, admissions), and margin by contract.
- Measure-level drill-downs: denominator completeness, data source reliability, and variance versus target. NCQA’s digital quality work is making automated measure calculation practical and auditable.
Advanced capabilities that add value
- Attribution reconciliation (monthly) with exception workflows.
- What-if modeling for contract scenarios (e.g., two-sided risk vs. upside only).
- Equity lensing to track disparities across SDOH groups.
Note: include confidence intervals and data-completeness scores on every executive dashboard so decisions aren’t made on fragile denominators.
Patient Engagement and Care Coordination in Value-Based Care Programs
Patients are the final mile. After all, engagement reduces utilisation and improves outcomes when it’s simple, timely, and relevant.
Tactics that work:
- Short, validated PROMs delivered by SMS or app use PROMIS or ICHOM sets for condition-specific tracking. Keep forms brief and tied to clinical decisions.
- Automated outreach for preventive care (screening reminders), medication adherence nudges, and post-discharge follow-ups.
- Remote patient monitoring (RPM) for chronic disease cohorts recent reviews show RPM can improve blood pressure control and other chronic outcomes when paired with care workflows.
- Social care referrals with closed-loop tracking so you can measure whether SDOH interventions actually reduce readmissions or ED use.
Care coordination tools:
- Shared care plans that multiple providers can see and update.
- Role-based task assignment (nurse, pharmacist, community health worker).
- Two-way secure messaging and clinician-viewable patient activity logs.
Metric to watch: percent of targeted patients with an active care plan and time from discharge to first follow-up contact.
Reducing Administrative Burden and Optimizing Workflows in Value-Based Care
Frontline adoption fails when a new system creates more clicks. Therefore, fix workflows first, then automate.
Practical steps:
- Embed tools in the EHR (SMART apps) so clinicians and care managers don’t toggle separate systems.
- Automate repetitive tasks: HEDIS data extraction, prior-auth document assembly and submission, and claims reconciliation where possible (use Da Vinci PAS and CMS prior-auth requirements to remove manual steps).
- Single sign-on & role-aware views reduce cognitive load and speed adoption.
- Measure staff time saved as part of your ROI case.
Example payoff: standardized discharge processes like AHRQ’s Re-Engineered Discharge (RED) have reduced 30-day readmissions by about 25% in studies. Process design plus software automation drives outcomes.
Continuous Improvement Through a Learning Health System in Value-Based Care
Treat VBC as an experiment: test, measure, refine.
How to operationalize learning:
- PDSA cycles for outreach scripts, RPM thresholds, and frequency of touchpoints.
- A/B operational experiments (different messages, different staffing models) and measure lift on the worklist.
- Model governance to detect drift in prediction models and retrain when necessary.
- Clinician feedback loops are built into dashboards so users can flag data errors or workflow issues.
Custom software should make experimentation cheap: feature flags, cohort attribution, and automatic metric calculation let you scale only what works.
Compliance and Data Security in Value-Based Care Implementation
Security and compliance are non-negotiable. So, the board and regulators will ask for evidence.
What boards should require:
- Annual HIPAA risk analysis and remediation plan; align controls to NIST SP 800-66. NIST’s 800-66r2 provides practical mapping to the HIPAA Security Rule.
- Least-privilege access, MFA, encryption in transit and at rest, immutable audit logs, and vendor SOC reports.
- Policies for TEFCA and information blocking compliance, where applicable.
Technical must-haves for software:
- Tokenization or PHI masking for analytics environments.
- Automated breach detection and tabletop exercise results as part of vendor selection.
- Consent and provenance tracking of who shared what and why, especially when pulling external clinicals via TEFCA.
Phased Rollouts and Staff Training for Value-Based Care Adoption
Don’t do everything at once. With this in mind, use a phased, measurable rollout.
Suggested phases:
- Phase 0 (0–90 days): governance, pick pilot contract & measures, readiness scan.
- Phase 1 (3–6 months): interoperability hub (Bulk FHIR + one claims feed), measure engine prototype, one SMART embedded app.
- Phase 2 (6–9 months): care management cockpit, attribution & HCC scoring in production, targeted RPM or PROMs pilot.
- Phase 3 (9–12 months): prior-auth pilot via FHIR, expand cohorts, show first quarterly results, and financials.
Training approach:
- Role-based training (clinicians vs. care managers vs. executives).
- Champions program identifies power users in each clinic to spread adoption.
- Weekly huddles using the software worklist to drive behavior change.
Measuring Outcomes and Refining Strategies in Value-Based Care
Your long-term credibility rests on measuring real outcomes and financial impact.
Key metrics to report monthly/quarterly
- Clinical: HEDIS/dQM rates, PROM improvement, readmissions, ED visits.
- Financial: shared savings, total cost of care per attributed patient, revenue at risk vs. protected.
- Operational: gaps closed, average time to close, prior-auth turnaround.
- Experience & equity: CAHPS composites and measurement by SDOH segment.
Use the results to renegotiate contracts, scale high-performing programs, and retire low-impact activities.
How Custom Software Ties Value-Based Care Implementation Together
Custom healthcare software is not just one piece of the puzzle; it’s the glue that makes the value-based care model actually work in day-to-day operations. Here’s how:
- Seamless Data Integration
Custom APIs and FHIR-based solutions connect disparate systems (EHR, claims, labs, telehealth, wearables) into one unified platform. No more silos. - Real-Time Analytics & Dashboards
Tailored dashboards show exactly the performance metrics you need: readmissions, quality scores, and patient outcomes, so executives and care teams always know where they stand. - Automated Compliance & Reporting
Built-in logic ensures regulatory compliance (HIPAA, CMS quality reporting, payer contracts) and generates reports without manual burden. - Personalized Patient Engagement Tools
From mobile apps to patient portals, custom solutions allow condition-specific reminders, care plans, and two-way communication with patients. - Workflow Optimization
Interfaces and workflows are designed around your clinical teams, not a generic vendor template, reducing clicks, eliminating duplicate entry, and saving provider time. - Care Coordination Hub
A central communication platform for multi-disciplinary teams, referrals, and patient updates, everyone stays aligned on the same care plan. - Scalability and Flexibility
As your organization takes on new payer contracts, new quality measures, or new patient populations, custom software adapts no waiting for vendor updates. - Built-In Continuous Learning
Feedback loops built into the system help organizations adjust quickly, embedding a “learning health system” culture with every new data point.
Want to see what this looks like in practice? Let’s talk.
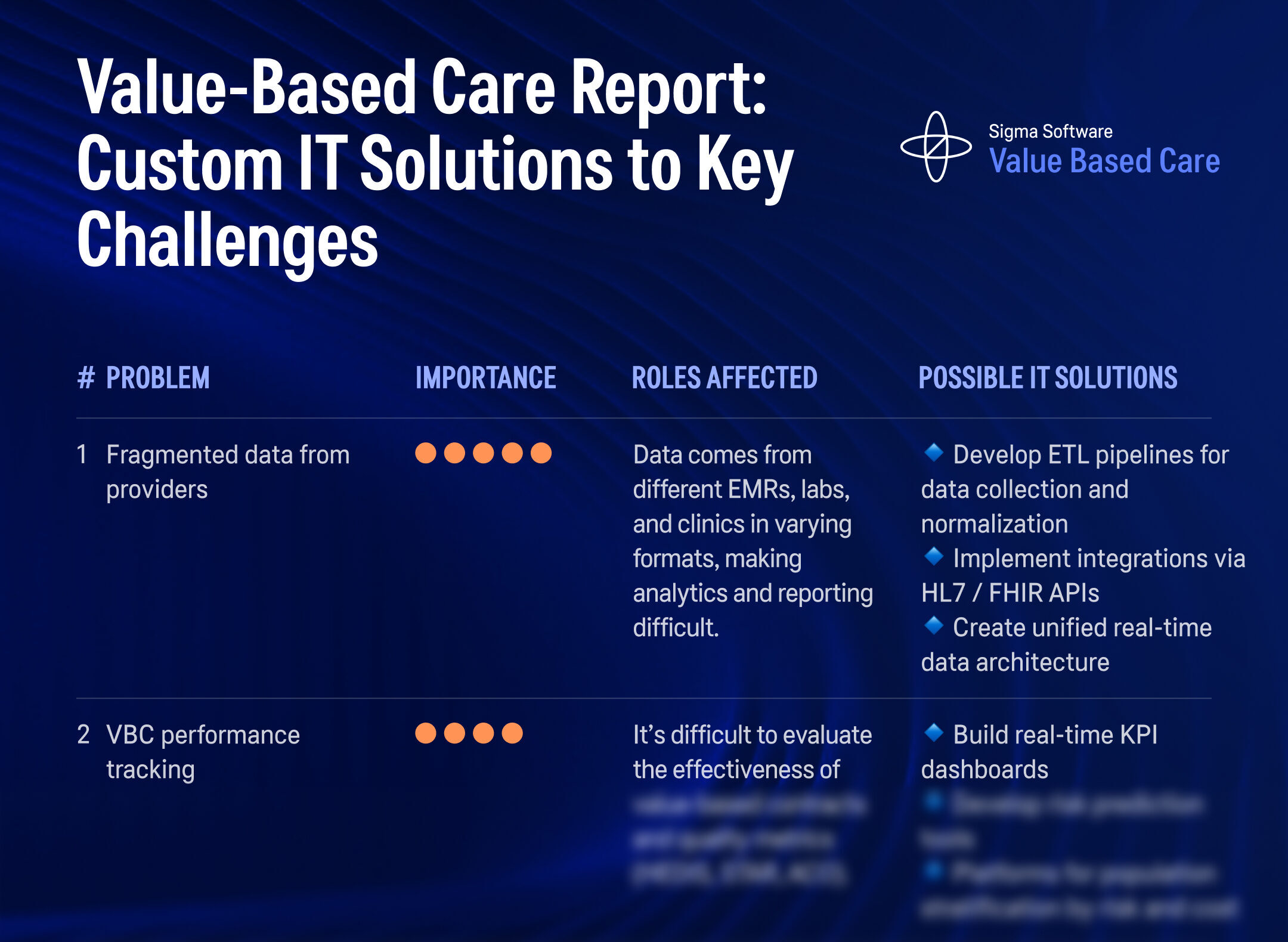
Anonymous Value-Based Care Insights: Key Challenges & IT Solutions
We conducted an anonymous research across healthcare and insurance organizations transitioning to Value-Based Care.
Discover the top challenges leaders face — from fragmented data and performance tracking gaps to ROI transparency — and explore proven IT solutions to overcome them.
Ready to Solve Your Value-Based Care Challenge?
Let’s talk about your unique workflows and design a custom digital health solution that supports outcome-based care, improves population health, and aligns with value-based reimbursement models.
Whether you’re navigating HEDIS metrics, improving care coordination, or optimizing performance-based contracts, we can help.
Build Your Custom Implementation Plan
Your implementation plan includes integrations, MVP timelines, and long-term support strategies. We build your value-based care solution around real workflows, compliance requirements, and measurable outcome goals.
Launch and Optimize for Outcome-Based Development
Our solutions combine predictive analytics, AI-driven clinical insights, and secure, interoperable data flows. Whether you need compliance tools, shared savings tracking, or a care coordination engine, we align it with your quality metrics, reimbursement goals, and care delivery model.
Ready to Improve Outcomes with Custom Value-Based Solutions?
We design and build custom software for value-based healthcare, built around your data, workflows, and objectives. Whether you need to unify data, support attribution, or track performance across contracts—we’re here to build what works.
Custom Software for Aesthetic Clinics: Overcoming Digital Growth Challenges
Solving the 5 Core Data Infrastructure Problems in Diagnostics
3 AI Execution Gaps Slowing Down Medical Distribution
Resolving Fragmented Clinical Data in Biotech
The 7 Core IT Engineering Bottlenecks in Clinical Stage Biotech (And How to Resolve Them)
Where AI Actually Works in Biotech: Clinical Trials, Genomics, and Drug Discovery
Stay in the loop with everything you need to know.